An enteric coating, also known as gastro-resistant coating is a barrier applied to oral medication that controls the location in the digestive tract where it is absorbed. The term “enteric” refers to the small intestine; therefore, enteric coatings resist breakdown of medication before it reaches the small intestine.
Enteric coatings are employed when the drug substance is inactivated or destroyed in the acid secretion of the stomach or is particularly irritating to the gastric mucosa or when bypass of the stomach substantially enhances drug absorption.
Early approaches to preparing enteric-dosage forms involved treating gelatin capsules with formalin or coating tablets with shellac. Both of these approaches were unreliable since the solubility of the membrane (which is responsible for the enteric effect) can be unpredictable.
Modern enteric coatings are usually formulated with synthetic polymeric material often referred to as polyacids. These polymers contain ionizable functional groups that render them water-soluble at a specific pH value.
Contents
Enteric coatings are applied to dosage forms for the following reasons:
Some of the key attributes of enteric coating materials include:
Cellulose acetate phthalate, also known as cellacefate is the oldest and most widely used synthetic enteric coating polymer. It was patented as an enteric agent in 1940 by Eastman Kodak Company. CAP is synthesized by reacting a partial acetate ester of cellulose with phthalic anhydride in the presence of a tertiary organic base such as pyridine, or a strong acid such as sulfuric acid.
In the resulting polymer, of the free hydroxyl groups contributed by each glucose unit of the cellulose chain, approximately half are acylated and one-quarter esterified with one of the two carboxylic acid groups of the phthalate moiety. The second carboxylic acid group being free to form salts and thus serves as the basis of its enteric character.
Because the degree of substitution can lead to changes in CAP properties, specifications for CAP composition have been established to ensure more uniform performance from batch to batch. According to United State Pharmacopoeia (USP) specifications, CAP should contain 21.5 – 26.0 % w/w acetyl content and 30.0 – 36.0 % w/w phthalyl groups on the cellulose backbone as calculated on an anhydrous basis.
CAP is insoluble in water, alcohols, hydrocarbons, and chlorinated hydrocarbons but soluble in ketones, ethers, alcohols, esters, and in certain solvent mixtures. It exhibits rapid dissolution at a pH > 6 and is relatively permeable to moisture and gastric juices. Due to its high moisture permeability, CAP is susceptible to hydrolytic decomposition.
Phthalic and acetic acid molecules may hydrolyze during storage and significantly compromise the degree of enteric protection that the film coating provides. The addition of a plasticizing agent has been shown to improve the water-resistance of CAP films.
CAP is compatible with most water-soluble and insoluble plasticizers with diethyl phthalate (DEP), tributyl citrate (TBC), triethyl citrate (TEC), tributyrin, and triacetin being the most commonly used; typically in the range of 25 – 35 % by weight of dry polymer. Like other phthalates, CAP is susceptible to hydrolysis under high temperature and humidity.
CAP is commercially available as a white powder from Eastman Chemical Co. A 30 % solids latex dispersion version of CAP (Aquacoat® CPD) is also available for aqueous enteric coating of tablets, beads, both hard and soft gelatin capsules.
Chemically this polymer bears a strong resemblance to CAP. It is formed by the same synthesis process as CAP with trimellitic anhydride as the substituent group in place of phthalic anhydride. Typical values for timellityl and acetyl substitution are 29.0 % and 22.4%, respectively.
Trimellitic anhydride contains an additional free carboxyl group over that of phthalic anhydride, and hence CAT contains a greater concentration of acidic groups for a given degree of substitution than CAP rendering it more soluble in aqueous media. Also, the pKa of CAT is between 4.1 and 4.3 which is slightly lower than CAP. With a relatively low pKa value and greater functional group concentration,
CAT is the most soluble enteric cellulose derivative with the onset of dissolution occurring at pH 4.7–5.0. This useful property makes CAT ideal for targeted drug release to the proximal regions of the small intestine.
CAT is commercially available as a white powder from Eastman Chemical Co. To obtain the best enteric coating results from aqueous processing, ammoniacal solutions of CAT in water are recommended. Plasticizer considerations for CAT are identical to that of CAP.
HPMCP is a white to slightly off-white, free-flowing flakes or granular powder with a slightly acidic odour and a barely detectable taste. It is a derivative of hydroxypropyl methylcellulose that is produced by the transesterification of hydroxypropyl methylcellulose with phthalic acid.
This polymer was first introduced in 1971 by the Shin-Etsu Chemical Company, Tokyo, Japan as a cellulose derivative for enteric coating. HPMCP has been admitted in the European and Japanese pharmacopoeias and included in the USP/NF under the name hypromellose phthalate. Depending on the degree of phthalyl substitution, HPMCP is soluble in aqueous media in a pH range of 5.0 – 5.5.
Read Also: Polymers used in immediate-release film coating
HPMCP is characteristically insoluble in gastric fluids but swellable and rapidly soluble in the upper intestine. It may be plasticized with diethylphthalate, acetylated monoglyceride or triacetin. Mechanically HPMCP is a more flexible polymer and on a weight basis will not require as much plasticizer as CAP or CAT.
HPMCP is insoluble in dichloromethane, methanol, isopropanol. ethyl acetate and ethanol but demonstrates desired solubility in acetone, tetrahydrofuran, mixtures of dichloromethane and methanol, mixtures of dichloromethane and ethanol and mixtures of acetone and methanol. The insolubility of this polymer in single-solvent system makes it challenging to conduct simple drug-compatibility studies and spray drying applications.
However, solvent mixtures can be effectively prepared for commercial spray-drying by using proper spray-drying optimization. These polymers remain chemically and physically stable at room temperatures for several years but are susceptible to hydrolysis under elevated temperatures and humidity conditions.
HPMCAS also known as hypromellose acetate succinate is a white to off-white powder or granules derived from HPMC by the esterification of free hydroxyl groups on the polymer backbone with acetic anhydride and succinic anhydride. It is commercially available in three grades (L, M & H), which correspond to pH-dependent release profiles of low pH (5.0), medium (5.5) and high (6.5) pH.
HPMCAS is insoluble in acidic media, yet soluble in neutral pH according to ionization of free carboxyl groups on the polymer backbone. It has been demonstrated to be more chemically stable than CAP and HPMCP as indicated by a substantial reduction in the evolution of free acid when stored at 60˚C and 100% relative humidity (RH).
HPMCAS has glass transition temperature ranging between 120°C -135°C according to polymer grade. Since HPMCAS is a relatively rigid polymer, plasticization is utilized to improve film flexibility and reduce cracking as well as to promote film formation from HPMCAS aqueous dispersions.
Polyvinyl acetate phthalate is a free-flowing white to off-white powder with a slight odour of acetic acid. It is a reaction product of phthalic anhydride, sodium acetate, and a partially hydrolyzed polyvinyl alcohol.
The onset of aqueous dissolution of PVAP begins at a pH of about 5.0 allowing for enteric release as well as the potential for targeted drug release to the proximal small intestine. Although structurally similar to CAP (containing the dicarboxylic phthalic acid in a partially esterified form),
PVAP is relatively more stable to hydrolysis than CAP due to its lower moisture permeability. It is compatible with several of the most common plasticizers; namely glyceryl triacetate, TEC, acetyl triethylcitrate, DEP, and PEG 400.
PVAP (Sureteric®) is commercially available from Colorcon as a complete preformulated coating system consisting of a powder blend of PVAP, plasticizers, and other functional ingredients intended for reconstitution in water for rapid coating dispersion production.
This group of polymers are widely used for enteric coating applications as they contain free carboxylic acid groups that are ionized whenever the pH of the environment exceeds 5.5. They are produced by an emulsion-polymerization process and were first introduced for enteric coating applications by Lehmann and Dreher in the mid-1960s.
Today, these enteric polymers are marketed most notably by Evonik (formerly known as Röhm GmbH) under the proprietary Eudragit brand name.
Several different types of Eudragit polymers with enteric release capabilities are commercially available in a wide range of different physical forms (aqueous dispersion, organic solution, granules and powders). The pH at which these polymers dissolve is dependent on the content of the carboxylic acid in the copolymer.
Methacrylic acid methylmethacrylate copolymers (Eudragit L and S), and methacrylic acid ethyl acrylate copolymer (Eudragit L30D) are the preferred choice of coating polymers for enteric formulations. They allow targeting of specific areas of the intestine.
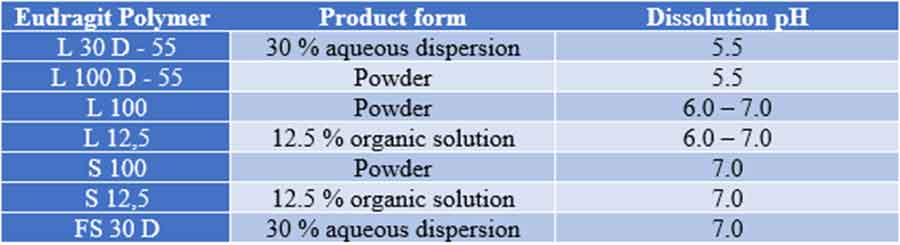
Eudragit polymers used in enteric coating and their dissolution pH
The functionality of enteric-coating polymers can be greatly affected by factors, such as:
Read Also: Examples of film-coated tablets
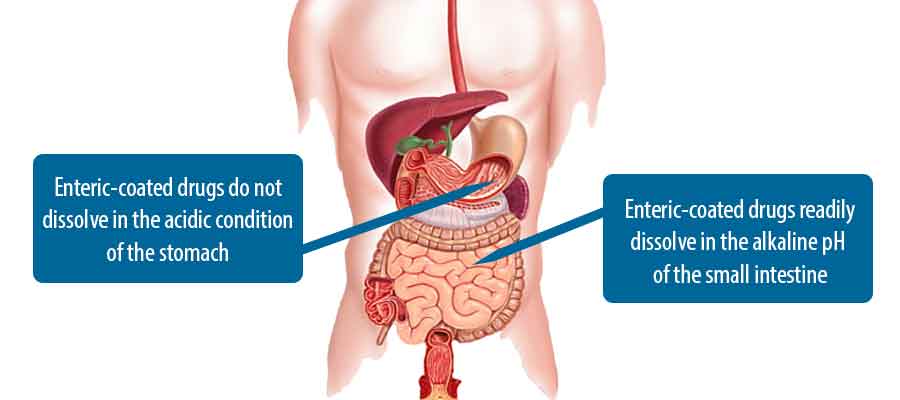
Enteric-coated tablets are compressed tablets coated with substances that do not dissolve in the acidic condition of the stomach but readily dissolves in the alkaline pH of the small intestine.
Most enteric coatings work by presenting a surface that is stable to highly acidic pH of the stomach but breaks down rapidly at a less acidic (relatively more basic) pH.
Enteric-coated tablets dissolve in the small intestine.
Enteric-coated tablets are swallowed whole with a full glass of water (8 ounces/ 240 millilitres).
Enteric-coated tablets should never be cut or crushed. They are designed to remain intact in the stomach (and exhibit low permeability to gastric fluids), but disintegrate and allow drug dissolution and absorption and/or effect once the dosage form reaches the small intestine.
Related keywords: enteric coating process, enteric coated tablets slideshare, disadvantages of enteric coated tablets, list of enteric-coated tablets, enteric coating defects, is enteric coating safe, enteric coated tablets pdf, enteric coating side effects